Turbt
TURBT (Transurethral Resection of Bladder Tumor) is a minimally invasive surgical procedure used to diagnose and treat tumors in the bladder. It is the standard procedure for managing bladder cancer, particularly non-muscle-invasive bladder cancer (NMIBC).
Indications
- Bladder tumors detected on imaging or cystoscopy.
- Hematuria (blood in urine) with suspected bladder pathology.
- Diagnosis and staging of bladder cancer.
Procedure
- Anesthesia:
- General or spinal anesthesia is used.
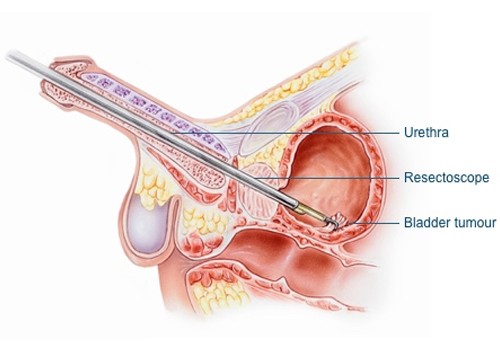
- Cystoscope Insertion:
- A resectoscope (a specialized cystoscope with a cutting loop) is inserted through the urethra into the bladder.
- Tumor Resection:
- Tumor tissue is resected using an electric loop or laser.
- The tissue is collected for pathological analysis.
- Cauterization:
- Bleeding areas are cauterized to prevent hemorrhage.
- Bladder Irrigation:
- Continuous saline irrigation is used to flush out blood clots and debris.
- Postoperative Steps:
- A catheter is placed temporarily to drain urine and allow bladder healing.
Key Purposes of TURBT
- Diagnosis:
- Provides tissue samples for histopathological examination to confirm cancer and determine its grade and stage.
- Treatment:
- Removes visible tumors for low-grade, non-invasive bladder cancers.
- Completes staging for invasive tumors to plan further treatment.
Postoperative Care
- Hospital Stay:
- Usually discharged within 1–2 days.
- Catheter Management:
- The urinary catheter remains for 1–2 days or longer if bleeding persists.
- Activity Restrictions:
- Avoid strenuous activities for 2–3 weeks.
- Hydration:
- Drink plenty of water to flush the bladder.
- Medications:
- Pain relievers, antibiotics, and medications to relax the bladder (if prescribed).
Complications
- Immediate:
- Bleeding (hematuria).
- Bladder perforation (rare, may require surgical repair).
- Infection (UTI).
- Delayed:
- Stricture formation in the urethra.
- Tumor recurrence (common with bladder cancer).
- Rarely, progression to invasive cancer.
Adjuvant Therapy
- For non-muscle-invasive bladder cancer (NMIBC):
- Intravesical therapy may follow TURBT to reduce recurrence risk:
- Chemotherapy (e.g., mitomycin C): Administered immediately post-surgery.
- Immunotherapy (e.g., BCG): Used in high-risk cases to stimulate immune response.
- Intravesical therapy may follow TURBT to reduce recurrence risk:
- For muscle-invasive bladder cancer (MIBC):
- Further treatments like radical cystectomy, systemic chemotherapy, or radiation therapy may be required.
Follow-Up
- Regular surveillance is crucial due to high recurrence rates in bladder cancer.
- Cystoscopy:
- Performed every 3–6 months initially, then annually for life.
- Imaging:
- CT or MRI to monitor the urinary tract.
- Urine Cytology:
- Evaluates for cancerous cells in urine.
Prognosis
- Non-invasive tumors:
- Excellent outcomes with TURBT and intravesical therapy.
- Invasive tumors:
- TURBT plays a diagnostic and staging role, with further treatment required for cure.
Conclusion
TURBT is a cornerstone procedure in the management of bladder tumors, providing both diagnostic and therapeutic benefits. It is often the first step in the comprehensive care of bladder cancer, followed by tailored treatments based on tumor pathology and stage.

